 ‘Until there is a change in the law, we’ll continue cutting’ – Dr I. Mushtaq (GOSH, UCL)
‘Until there is a change in the law, we’ll continue cutting’ – Dr I. Mushtaq (GOSH, UCL)
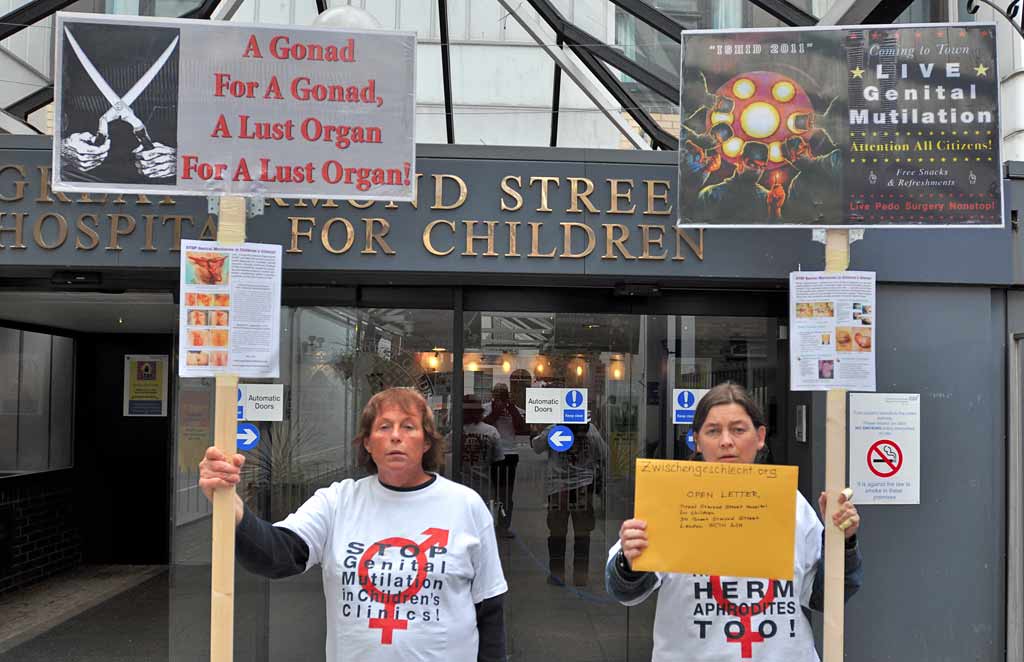
Photo: Nonviolent intersex protest @ Great Ormond Street Hospital for Children, 18.09.2011
>>> Press Release 09.06.2016: “IGM on the NHS” – UNCRC reprimands UK + Nepal
>>> Press Relase 25.05.2016: “UN to question UK for Intersex Genital Mutilations”

![]() This week it’s the turn of the UK to be questioned over Intersex Genital Mutilations at the 72nd Session of the UN Committee on the Rights of the Child (CRC) on Mon 23 May 15–18h CET [UK: 2-5pm] + Tue 24 May 10–13h CET [UK: 9am-noon]. >>> watch live!
This week it’s the turn of the UK to be questioned over Intersex Genital Mutilations at the 72nd Session of the UN Committee on the Rights of the Child (CRC) on Mon 23 May 15–18h CET [UK: 2-5pm] + Tue 24 May 10–13h CET [UK: 9am-noon]. >>> watch live!
UN-CRC recognises IGM as a ‘harmful practice’ (like FGM) and as ‘violence against children’, has recently reprimanded Ireland, France, Chile and Switzerland, and only last week questioned Nepal over IGM practices.
>>> StopIGM.org is reporting live from the 72nd session in Geneva, expecting tough questions also for the UK, and both the UK and Nepal to be reprimanded by June 3rd9th.
While the Government and the NHS are quick to deny the ongoing practice, a collaborative Intersex NGO report to the Committee documents damning evidence on the most common forms of IGM and moving testimonies by IGM survivors in the UK:
 NGO Report to the 5th Periodic Report of the United Kingdom on the Convention on the Rights of the Child (CRC)
NGO Report to the 5th Periodic Report of the United Kingdom on the Convention on the Rights of the Child (CRC)
Compiled by:
StopIGM.org • ISUK • OII-UK • UKIA
Some of the shocking evidence:
‘Until such time as there is a change in the law, we remain happy to undertake clitoral reduction surgery’ – Dr Imran Mushtaq (GOSH, UCL)
 UK government bodies, while admitting to the harm done by IGM practices, are quick to actively shield IGM perpetrators from human rights criticism by simply declaring the ongoing practice in the UK a thing of the past:
UK government bodies, while admitting to the harm done by IGM practices, are quick to actively shield IGM perpetrators from human rights criticism by simply declaring the ongoing practice in the UK a thing of the past:
“Intersex people are born with ambiguous primary physical sexual characteristics. Until recently they would usually undergo genital surgery at a young age to given them characteristics which are clearly either male or female. Medical professionals are now more likely to advise waiting until the child is older and able to provide informed consent to surgery, because of the implications surgery can have on future health and function.” – House of Commons, Women and Equalities Committee (2016), p. 5 (PDF)
The 2016 denial by above Women and Equalities Committee is remarkably similar to the below 2011 denial issued by the Great Ormond Street Hospital for Children GOSH, once more framing intersex human rights concerns as mere “different opinions”:
“GOSH […] recognise[s] that in the past such surgeries were carried out and the difficulties this has caused. We would like to reassure you that in advanced centres such as our own your concerns have been heard and influence our decision making process. Generally families are happy with the treatments now offered […]. As with any area of medicine with difficult ethical balances to strike on when and when not to offer treatment, this topic brings out a wide spectrum of opinion and we recognise the right of those with different opinions to express them.” – Great Ormond Street Hospital for Children NHS Foundation Trust (2011, PDF)
On the other hand, the “Society for Endocrinology UK guidance on the initial evaluation of an infant or an adolescent with a suspected disorder of sex development (Revised 2015)” generally advocates early unnecessary surgeries as legitimate, framing the human rights issues involved as mere “controversies”:
“Some parents may consider early genital surgery as a mechanism that could possibly protect their child from the risk of future stigma. This will require a thorough discussion with several members of the MDT [= multidisciplinary] team including the clinical psychologist, surgeons, gynaecologist and nurses so that the parents are fully informed of the controversies around undertaking or withholding early genital surgery.” – Faisal et al., Clinical Endocrinology (2016) 84, 771–788 (PDF)
Above “guidance” remains remarkably similar to the 2011 “best practice by a multidisciplinary team (MDT) dedicated to children with DSD” as promoted by paediatric urologist Dr Imran Mushtaq (Great Ormond Street Hospital for Children NHS Foundation Trust / Senior Lecturer Institute of Child Health, UCL London), published around the same time as the above 2011 GOSH denial and again framing intersex human rights concerns as mere “controversy” and “debate”:
“There is no subject that creates more controversy and debate than that relating to ‘feminising’ genital surgery in infants and children with DSD. […]”
“Many parents of children with DSD continue to express deep concerns about the appearance of the genitalia and these concerns need to be taken seriously and managed in an appropriate manner. […]”
“Clitoral surgery is generally considered when the clitoris is larger than ‘normal’. […] ”
“In girls with severe clitoral enlargement we remain happy to undertake clitoral reduction surgery, provided the family are fully informed and cognisant of the potential risks and benefits.”
“Until such time as there is a change in the law, parents will continue to have the right to decide if their child should or should not have genital surgery in infancy or childhood. […]” – Dr Imran Mushtaq, “Surgery in infants and children with DSD” (2011, PDF)
Accordingly, to this day the NHS continues to facilitate and pay for IGM Type 2: “Feminising Genital Surgeries”, including involuntary, unnecessary clitoral surgery on children 0–14 years on a regular basis – despite all ethics and human rights “controversy and debate”:

Similar findings are referenced in the report regarding IGM Type 3: Sterilising Procedures and IGM Type 1: “Masculinising Genital Surgeries”.
Thus the UK is in breach of its obligation to take effective legislative, administrative, judicial or other measures to prevent harmful practices (Art. 24 para. 3 CRC in conjunction with CRC/CEDAW Joint General Comment No. 18/31 “on harmful practices”), as well as of its obligations under Articles 2, 3, 6, 8, 12, 16, 19, 23, 24.1, 34, 36, and 37 of the Convention on the Rights of the Child (see below p. 53–58).
Also in the UK, victims of IGM practices encounter severe obstacles in the pursuit of their right to redress, fair and adequate compensation, including the means for as full rehabilitation as possible.
Further the UK’s efforts on education and information regarding the human rights aspects of IGM practices in the training of medical personnel are grossly insufficient with respect to the treatment of intersex people.
 Intersex Genital Mutilations in the UK: 2016 UN-CRC Report
Intersex Genital Mutilations in the UK: 2016 UN-CRC Report
Human Rights Violations Of Persons With Variations Of Sex Anatomy
IGM – Most Common Forms • What is Intersex? • A Harmful Practice
>>> Download (PDF 3.60 MB)
See also:
• 12 Verdicts by UN Treaty Bodies Condemning IGM – And Counting …
• UN Committee for the Rights of the Child (CRC) 2015: IGM = Harmful Practice
• UN Committee against Torture (CAT) 2015: IGM = Inhuman Treatment or Torture
• UN Human Rights Committee (HRCttee) to examine IGM Practices
• UN Committee on the Rights of Persons with Disabilities (CRPD) condemns IGM
• Historic 56th Session of Committee against Torture reprimands 4 Governments over IGM
• CAT 2011: Germany must investigate IGM practices and compensate survivors!
 Intersex Genital Mutilations • 17 Most Common Forms
Intersex Genital Mutilations • 17 Most Common Forms
Human Rights Violations Of Children With Variations Of Sex Anatomy
IGM – Historical Overview • What is Intersex? • How Common is IGM?
>>> Download PDF (3.65 MB) >>> Table of Contents

![]() Eliminating IGM practices by holding the perpetrators accountable via well-established applicable human rights frameworks, including Inhuman Treatment and Harmful Practices – Presentation @ UN expert meeting on Intersex Human Rights
Eliminating IGM practices by holding the perpetrators accountable via well-established applicable human rights frameworks, including Inhuman Treatment and Harmful Practices – Presentation @ UN expert meeting on Intersex Human Rights
>>> Download PDF (831kb)